Post written by Christopher W. Woodward, LAC, Substance Abuse Specialist
Post written by Christopher W. Woodward, LAC, Substance Abuse Specialist
September is Recovery Month, and this one is marked by 2020 and COVID-19. We find that many of our co-workers, family members and community members have moved toward substance use in the past several months to cope with the stress and ongoing fear of the unknown.
In continuing to contact clients through telehealth services, we have been speaking with many clients from diverse backgrounds and support systems and have come to the realization that the COVID-19 protocols had in many cases drastically changed clients’ positive coping strategies for their recovery efforts.
The gym had closed where clients would exercise and burn off calories and stress. The parks have had to shut down, which was an excellent way for clients and their children to play and have social interactions with others. The community support groups had to move from face-to-face to virtual interactions. The workplace has drastically changed, and some of our clients are having hours reduced, while still others are out of work completely.
As we review much of the recovery plans that we had worked up over the past years it appears that the primary focus points were now not accessible for our clients. This appears to be a recipe for relapse and troubles. In my mind, this can be used as a positive if we can keep and gain recovery in a situation where our primary coping skills are not easily accessed then we can maintain that recovery in many other circumstances.
At this point most of you are saying good, you know the problem, now where are the answers?
The good news is that as always, in recovery, we adapt, we learn, and we find a new way of doing things. I have seen in our clients a resiliency to recover and open doors that were once shut to family and friends. Many of us are now near our family in some cases this is a positive; in others there are amends and positive steps that can be taken to open the lines of communication that have been shut off for years. I always find myself saying, “take a breath,” “breathe,” and “practice openness to new ideas.” Below you will find three ideals on how to find a new way to recovery.
-Put on your Pants –
 I was recently talking to a parent about recovery and found myself giving the analogy of putting on your pants. We all do it, right? So, it is a common experience. We go left leg first or some are right leg first, a few of you might run down the bed and jump into your pants– firefighter style. But we do it, well I hope we do it. That might be my first point if you have not put on your pants in a while and gone out into the world because of COVID-19. This may be your first step. Take a walk, go smell the flowers, sit on a bench, listen to the birds, find peace in your surroundings. Of course take precautions and allow space for yourself and others, but simply getting outside and knowing that the trees and the grass are still growing, the wind still blows and the sun makes its daily rounds can bring us back to a grounded state of mind and have assurance that this too will pass.
I was recently talking to a parent about recovery and found myself giving the analogy of putting on your pants. We all do it, right? So, it is a common experience. We go left leg first or some are right leg first, a few of you might run down the bed and jump into your pants– firefighter style. But we do it, well I hope we do it. That might be my first point if you have not put on your pants in a while and gone out into the world because of COVID-19. This may be your first step. Take a walk, go smell the flowers, sit on a bench, listen to the birds, find peace in your surroundings. Of course take precautions and allow space for yourself and others, but simply getting outside and knowing that the trees and the grass are still growing, the wind still blows and the sun makes its daily rounds can bring us back to a grounded state of mind and have assurance that this too will pass.
Yes, back to the pants, I was talking to the parent of a client, and they were noting that they just did not understand how their child was making such poor choices where substances were concerned. I asked in a coy manner, which leg do you start with when you put on your pants. Through the puzzled looks the parents noted that they did not remember. I said but you do it every day, maybe sometimes more than once. It is an action that you should remember, correct? This for some is an action much like substance use. A task for many reasons that is frequently done and has become due to the reinforcement of the substance almost muscle memory. Much like putting on our pants.
Remembering that our actions and repeated actions where substances are involved has been reinforced chemically over time is important. Then to further confound the parent, I asked them to try something new, to put on their pants opposite leg first next time. The predictable outcome is that they might fall over, or at least lose balance, and create thought, to think long and hard about the first leg to go in. That is like asking our friends and family to try recovery. We are using a different set of skills than we had when we were in our dependency and need to re-work the thought process so that recovery becomes as much muscle memory as our unnoticeable tasks.
-Limit the Noise-
 This Recovery Month, many of us are attempting to re-engage into society and find the normalcy of life. This month feels a bit to me like walking in the fog. For many of us, we have our resolutions, recovery goals and direction in life set before us. However, to get there with all the shadows and obstacles in our paths it is hard for us to identify them through the mist. These obstacles or impending shadows can be our own guilt, shame and failures. The mist (noise) however, for most of us, in and of itself is not harmful to us, it is the obstacles we don’t see that is in our path or at our feet that can cause us to trip and fall. The mist, like the noise, in our life dulls one of our five senses and can limit our sensory intake and literally create a blind spot for us.
This Recovery Month, many of us are attempting to re-engage into society and find the normalcy of life. This month feels a bit to me like walking in the fog. For many of us, we have our resolutions, recovery goals and direction in life set before us. However, to get there with all the shadows and obstacles in our paths it is hard for us to identify them through the mist. These obstacles or impending shadows can be our own guilt, shame and failures. The mist (noise) however, for most of us, in and of itself is not harmful to us, it is the obstacles we don’t see that is in our path or at our feet that can cause us to trip and fall. The mist, like the noise, in our life dulls one of our five senses and can limit our sensory intake and literally create a blind spot for us.
I look at the “busyness” of our world and our involvement with social media and the access we have to information can be seen as mist or fog. All this information can blur our thoughts and our vision for the direction that we want to go. I many times have picked up my phone to make a call or answer an email and have gone down “the rabbit hole” as it were. I had my mind distracted and lost time by simply clicking a link to a message or looking at a text. This seems all to simple for most of us to get lost in the mist of the multitude of voices clamoring for our attention.
I have had multiple conversations with clients that they took a side-step toward relapse by answering a message from an “associate” or family member that “did not have my best interest in mind.” These contacts can also become the mist and fog of recovery; they are out there and can cloud us from where we want to go and send us backward in our recovery. Remember the prayer “God, grant me the serenity to accept the things I cannot change, courage to change the things I can, and wisdom to know the difference.” For me, wisdom is making it through the mist/fog without bumping the trees.
Discerning what is a “recovery” thought from a “using” thought is our greatest way to limit the noise of our mind, body and untimely our soul. I know that the noise and mist will always be there to dull my perceptions of others and society in general. I have to take control of these thoughts and actions and find wisdom in myself to limit the contacts, the apps and the distractions so that I can find my way down the path for myself.
-Work the Problem –
Let us remember that our recovery, family and life in general are not a finished work. The problems that we have today can become fading memories. Remember, Thomas Edison, the inventor of the light bulb failed a thousand times before he came up with the invention that most of us take for granted every day. Each morning I flip a switch and can instantly see where I am going mist or no mist. I benefit from the inventor’s failures and eventual success each day. This is a great thing to keep in mind that my problems are temporary if I work on them every day.
Walking was a big deal when I was an infant, and I can do that pretty well most days, even putting on my pants in my toddler years was troublesome. Words, math, kissing, all of these I learned along the way, and I have the bumps and the bruises to show for it. The same goes with recovery. The more we work the problem the better we understand ourselves and our triggers.
I need to keep working my problems and overcome each failure so that someday I will take for granted all of the lessons of recovery and life that I have learned in the past. They happen in the same form as when I click the switch to wake up each morning. Keeping in the front of my mind the thought that I am an evolving person that is teachable, allows me to look at problems differently. I can see that my interactions with others are not always perfect, and I can take responsibly for my actions and failures in the relationships. This opens the relationship up to collaboration when I partner with others in recovery. The problem can be worked on because it is not about the other person or my failures, it is about making progress on a mutual goal.
– Final Thought –
Momentum can be our greatest ally or difficult to overcome. Depending on which way it is swaying at the time. COVID-19 appears to have pulled the momentum in a way that it has never gone before, and we need to as persons in recovery and family of persons in recovery to learn a new way to sway the momentum back in our favor. Hopefully, these tips will be an avenue to making each day that much more successful.
HPC offers Substance Abuse services. For more information, call 913-730-3664.

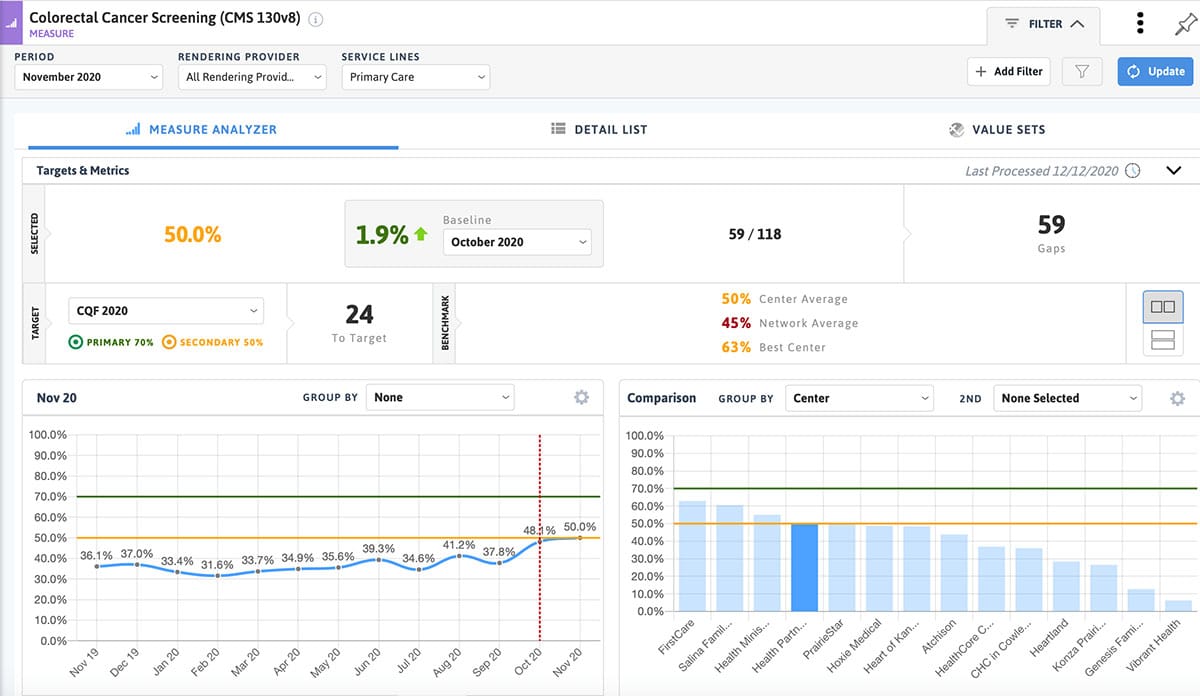
 About 24 percent of our medical patients at Health Partnership Clinic have one or more chronic diseases such as diabetes, depression and hypertension. Our providers and support staff partner with these patients to help manage their disease to ensure optimal outcomes.
About 24 percent of our medical patients at Health Partnership Clinic have one or more chronic diseases such as diabetes, depression and hypertension. Our providers and support staff partner with these patients to help manage their disease to ensure optimal outcomes.

 Flu infection rates were dramatically low during the 2020-2021 season, even though the number of tests that were done was high. Scientists at the CDC believe this is due to the measures put in place for COVID-19, such as hand washing, physical distancing, school and other closures, increased ventilation in closed spaces, staying home and wearing masks. These same practices can lower your chance of getting a cold, the flu and COVID-19.
Flu infection rates were dramatically low during the 2020-2021 season, even though the number of tests that were done was high. Scientists at the CDC believe this is due to the measures put in place for COVID-19, such as hand washing, physical distancing, school and other closures, increased ventilation in closed spaces, staying home and wearing masks. These same practices can lower your chance of getting a cold, the flu and COVID-19. By
By  Ethnicity, sexual orientation, gender identity—all of these conspire to make certain populations at risk. I was shocked to find that there is a 50 percent lifetime risk of HIV of black men who have sex with men (MSM). White MSM also have increased risk, as opposed to heterosexual couples. Some sexual activity is riskier than others. Receptive anal sex is the highest risk, followed by receptive vaginal intercourse. Women who have sex with women (WSW) HIV transmission is practically nonexistent. Condom use and other barrier methods like dental dams can dramatically decrease risk. Condoms should be used for all kinds of sex.
Ethnicity, sexual orientation, gender identity—all of these conspire to make certain populations at risk. I was shocked to find that there is a 50 percent lifetime risk of HIV of black men who have sex with men (MSM). White MSM also have increased risk, as opposed to heterosexual couples. Some sexual activity is riskier than others. Receptive anal sex is the highest risk, followed by receptive vaginal intercourse. Women who have sex with women (WSW) HIV transmission is practically nonexistent. Condom use and other barrier methods like dental dams can dramatically decrease risk. Condoms should be used for all kinds of sex. Needle exchange programs and harm reduction strategies can help. Mother-baby transmission (perinatal) is becoming increasingly rare as HIV screening is routine, and anti-retroviral therapy during pregnancy is increasingly effective at preventing perinatal infection.
Needle exchange programs and harm reduction strategies can help. Mother-baby transmission (perinatal) is becoming increasingly rare as HIV screening is routine, and anti-retroviral therapy during pregnancy is increasingly effective at preventing perinatal infection.
 Post written by
Post written by 

 By
By 
 As a general rule, I only like one combination product to be used at a time, like Dayquil in the morning, Nyquil in the evening, in addition to plain ibuprofen for muscle aches. It is too easy to take too much of one individual medication if you take multiple combination products. Dayquil and Nyquil both contain acetaminophen, so if you take additional acetaminophen on top of that you can damage your liver. Advil/ibuprofen is in a different drug class than Tylenol/ibuprofen, so it is fine to combine ibuprofen doses with Dayquil/Nyquil. Easiest thing to do is to ask a pharmacist when you are there at the pharmacy!
As a general rule, I only like one combination product to be used at a time, like Dayquil in the morning, Nyquil in the evening, in addition to plain ibuprofen for muscle aches. It is too easy to take too much of one individual medication if you take multiple combination products. Dayquil and Nyquil both contain acetaminophen, so if you take additional acetaminophen on top of that you can damage your liver. Advil/ibuprofen is in a different drug class than Tylenol/ibuprofen, so it is fine to combine ibuprofen doses with Dayquil/Nyquil. Easiest thing to do is to ask a pharmacist when you are there at the pharmacy! Deciding when to go to the ER, can be tricky. Any of my patients telling me they feel short of breath is always concerning. A patient that is struggling to breathe, using chest and throat muscles to breathe, or running out of air with only talking always gets me worried. A fever that cannot be controlled at home with antipyretics such as Tylenol/acetaminophen or Advil/ibuprofen, or a temperature over 103.5 degrees Fahrenheit is also a good reason to go to the ER. A child that is not drinking normally and has dry mucous membranes is also concerning, and if the parent is concerned for their child, their instincts are usually right on the nose. However, if you have a slight sore throat and/or manageable symptoms, stay home and call the clinic!
Deciding when to go to the ER, can be tricky. Any of my patients telling me they feel short of breath is always concerning. A patient that is struggling to breathe, using chest and throat muscles to breathe, or running out of air with only talking always gets me worried. A fever that cannot be controlled at home with antipyretics such as Tylenol/acetaminophen or Advil/ibuprofen, or a temperature over 103.5 degrees Fahrenheit is also a good reason to go to the ER. A child that is not drinking normally and has dry mucous membranes is also concerning, and if the parent is concerned for their child, their instincts are usually right on the nose. However, if you have a slight sore throat and/or manageable symptoms, stay home and call the clinic!